
인슐린 디터머의 체중효과
제2형 당뇨병 환자의 치료에 있어서 전통적으로 경구용혈당강하제가 일차 약물로 이용되고 있으나 점진적인 베타세포의 기능 감소가 진행되면서 경구용혈당강하제 외에도 인슐린의 사용이 추가적으로 필요하게 된다1.
이전에는 인슐린 요법이 혈당강하를 위해 가장 마지막 단계의 선택으로 간주되었으나 최근 여러 연구들은 제2병 당뇨병의 초기 단계에 적극적인 인슐린 사용을 통해 베타세포의 기능을 오래 보존하고2 장기적으로 합병증의 발생을 감소시켜 조기인슐린 치료의 중요성이 부각되고 있다3-5.
제2형 당뇨병 환자에게서 인슐린 치료는 대개 기존의 경구용혈당강하제에 인슐린 글라진이나 인슐린 디터머와 같은 지속형 인슐린을 추가하여 시작된다. 인슐린은 대표적인 동화작용을 갖는 호르몬으로 사용시 체중증가 효과를 동반하게 되는데 일반적으로 제 2형 당뇨병 환자가 6개월 동안 인슐린 치료를 하게 되면 평균 8.7kg 정도 몸무게가 증가하는 것으로 알려졌다6.
특히 인슐린저항성이 매우 심한 제2형 당뇨병 환자에게 혈당을 떨어뜨릴 목적으로 인슐린을 투여 시 더욱 많은 양의 인슐린을 투여하는 경우가 흔히 발생하며, 특히 환자가 적절한 식사요법과 운동요법을 함께하지 않은 경우 과도한 인슐린 사용으로 인하여 지속적인 인슐린 투여량의 증가는 더 많은 체중증가(특히 내장지방의 증가)로 이어지는 악순환이 생기게 된다7-10.
이러한 현상은 최근 적극적인 치료(주로는 인슐린 사용)를 통하여 혈당을 낮춘 제2형 당뇨병 환자에게서 심혈관합병증으로 이한 사망률을 뚜렷하게 감소시키지 못했던 ACCORD, ADVANCE, VADT와 같은 여러 대규모 연구들의 공통된 설득력있는 원인으로 제시된다. 따라서 제2형 당뇨병 환자의 치료는 단지 목표 혈당의 달성만이 아니라 생활습관 개선을 통해 여러 심혈관계의 위험인자를 최적의 상태로 만드는데 목표를 두어야 한고 이러한 기초환경이 이루어진 상태에서 적절한 약물요법이 이루어져야 하며 인슐린을 사용하는 환자의 경우 더욱 그 중요성이 크겠다.
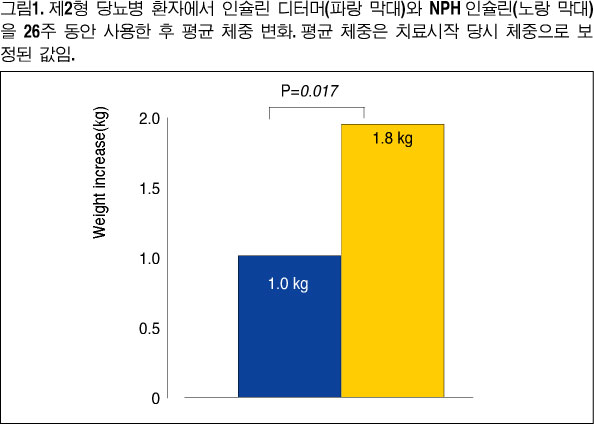
인슐린 글라진과 더불어 많이 사용되고 있는 지속형 인슐린인 디터머는 24시간의 혈당 강하 효과 외에도 혈당의 변동 폭이 작고 체중 증가가 상대적으로 다른 인슐린에 비해 적은 것으로 알려져 있다. 제2형 당뇨병 환자들을 대상으로 26주의 연구기간에서 인슐린 디터머는 중간형 인슐린(NPH, neural protamine hagedorn)에 비해 비슷한 혈당 조절 효과에도 불구하고 저혈당 발현이 적으며 체중 증가(+1.0 kg)가 적게 나타났으며
11(그림1), 비만한 제2형 당뇨병 환자에게서도 비슷한 결과를(+0.4 kg) 보였다12. 또한 기존에 경구용혈당강하제와 함께 NPH 인슐린 또는 인슐린 글라진을 사용 중인 제2형 당뇨병 환자에서 기존의 인슐린을 디터머로 교체하는 경우 평균 0.9 kg의 체중 감소가 나타났다13.
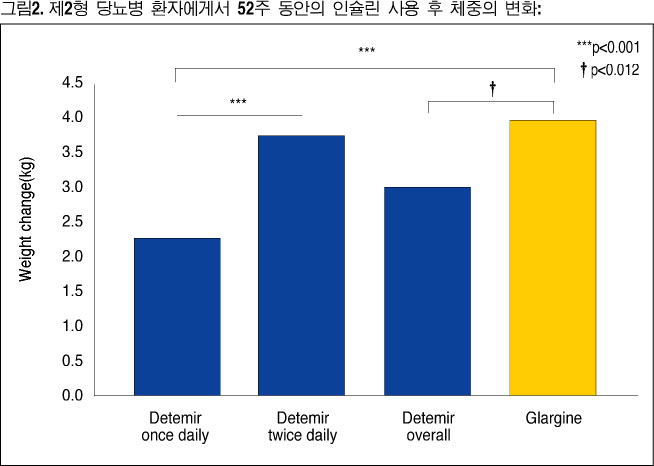
경구용혈당강하제를 사용 중인 제2형 당뇨병 환자에게 인슐린 글라진 또는 디터머를 52주 동안 사용한 연구결과에서 유사한 혈당 강하효과에도 불구하고 인슐린 디터머는 글라진에 비해 체중증가가 적은 것으로 나타났다14(그림2).
저혈당이 빈번히 나타나는 경우 혈당을 이를 회복하기 위하여 식사 사이에 간식 섭취가 늘어나기 때문에 체중의 증가가 나타날 수 있다. 인슐린 디터머는 다른 인슐린에 비해 저혈당이 적게 나타나는데 이 때문에 다른 인슐린에 비해 체중증가가 적다는 의견도 있으나15 인슐린 디터머 자체의 고유한 기전이 있기 때문일 것이라는 의견도 있다16.
인슐린 디터머가 체중증가가 적은 기전은 아직까지 잘 밝혀지지는 않았으나 임상전연구에서 나타난 결과로 추측하는 바는 인슐린 디터머가 말초조직 보다 간에 더 큰 효과를 보이고17 뇌에 작용하여 식욕을 억제하는 효과를 보이기 때문이다18.
인슐린 디터머와 같이 사용 후 체중증가가 적은 지속형 인슐린은 제2형 당뇨병 관리에 있어서 중요한 장점이 될 수 있을 것이다. 이 제제가 앞으로 당뇨병치료에서 차지할 역할에 대해 기대가 큰 것도 바로 이 때문일 것이다.
1. Barnett AH, Capaldi B, Davis-Lyons M et al. Expert opinion statement on the use of insulin therapy in patients with type 2 diabetes in primary care. Pract Diabetes Int 2003; 20: 97-102.
2. Alvarsson M, Sundkvist G, Lager I et al. Beneficial effects of insulin versus sulphonylurea on insulin secretion and metabolic control in recently diagnosed type 2 diabetic patients. Diabetes Care 2003; 26: 2231-2237.
3. Turner RC, Holman RR,
4. Ohkubo Y, Kishikawa H, Araki E et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulindependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract 1995; 28: 103-117.
5. Gaster B, Hirsch IB. The effects of improved glycemic control on complications in type 2 diabetes. Arch Intern Med 1998; 158: 134-140.
6. Russell-Jones D, Khan R. Insulin-associated weight gain in diabetes--causes, effects and coping strategies.Diabetes Obes Metab. 2007;9:799-812.
7. Douek IF, Gale EAM. The problem of weight gain on insulin. In: Barnett AH., ed. Insulin Made Easy.
8. Caro JF. Clinical review 26: insulin resistance in obese and nonobese man. J Clin Endocrinol Metab 1991; 73: 691-695.
9. Gumbiner B, Battiwalla M. Obesity and type 2 diabetes mellitus: a treatment challenge. Endocrinology 2002;
10. Sowers JR. Obesity as a cardiovascular risk factor. Am J Med 2003; 115: 37-41.
11. Haak T, Tiengo A, Draeger E, Suntum M, Waldhausl W. Lower within-subject variability of fasting blood glucose and reduced weight gain with insulin detemir compared to NPH insulin in patients with type 2 diabetes. Diabetes Obes Metab. 2005;
12. Fajardo Montanana C, Hernandez Herrero C, Rivas Fernandez M. Less weight gain and hypoglycaemia with once-daily insulin detemir than NPH insulin in intensification of insulin therapy in overweight Type 2 diabetes patients: the PREDICTIVE BMI clinical trial. Diabet Med. 2008;25:916-23.
13. Meneghini LF, Rosenberg KH, Koenen C, Merilainen MJ, Luddeke HJ. Insulin detemir improves glycaemic control with less hypoglycaemia and no weight gain in patients with type 2 diabetes who were insulin naive or treated with NPH or insulin glargine: clinical practice experience from a German subgroup of the PREDICTIVE study. Diabetes Obes Metab. 2007;9:418-27.
14. Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes.Diabetologia. 2008;51:408-16.
15. Davies M, Derezinski T, Kim H, Clauson P. No correlation between weight gain and number of hypoglycemic events in patients with type 2 diabetes treated with insulin detemir as compared to NPH insulin. Diabetes 2006; 55: A466.
16. Davies MJ, Derezinski T, Pedersen CB, Clauson P. Reduced weight gain with insulin detemir compared to NPH insulin is not explained by a reduction in hypoglycemia.Diabetes Technol Ther. 2008;10:273-7.
17. Hordern SVM, Wright JE, Umpleby AM, Shojaee-Moradie F, Amiss J, Russell-Jones DL. Comparison of the effects on glucose and lipid metabolism of equipotent doses of insulin detemir and NPH insulin with a 16-h euglycemic clamp. Diabetologia 2005; 48: 420-426.
18. Hennige AM, Sartorius T, Tschritter O et al. Tissue selectivity of insulin detemir action in vivo. Diabetologia 2006; 49: 1274-1282.